Shoulder pain is one of the most common reasons people visit a doctor or physical therapist. It doesn’t always come from a fall or a sudden injury. Often, it creeps in slowly-maybe you started carrying groceries differently, or your job requires you to reach overhead, or you’ve been sleeping on that side for years. The real culprits? Two closely linked problems: rotator cuff issues and subacromial bursitis. And the good news? Most cases don’t need surgery. With the right approach, you can get back to lifting, sleeping, and reaching without pain.
What’s Actually Going On in Your Shoulder?
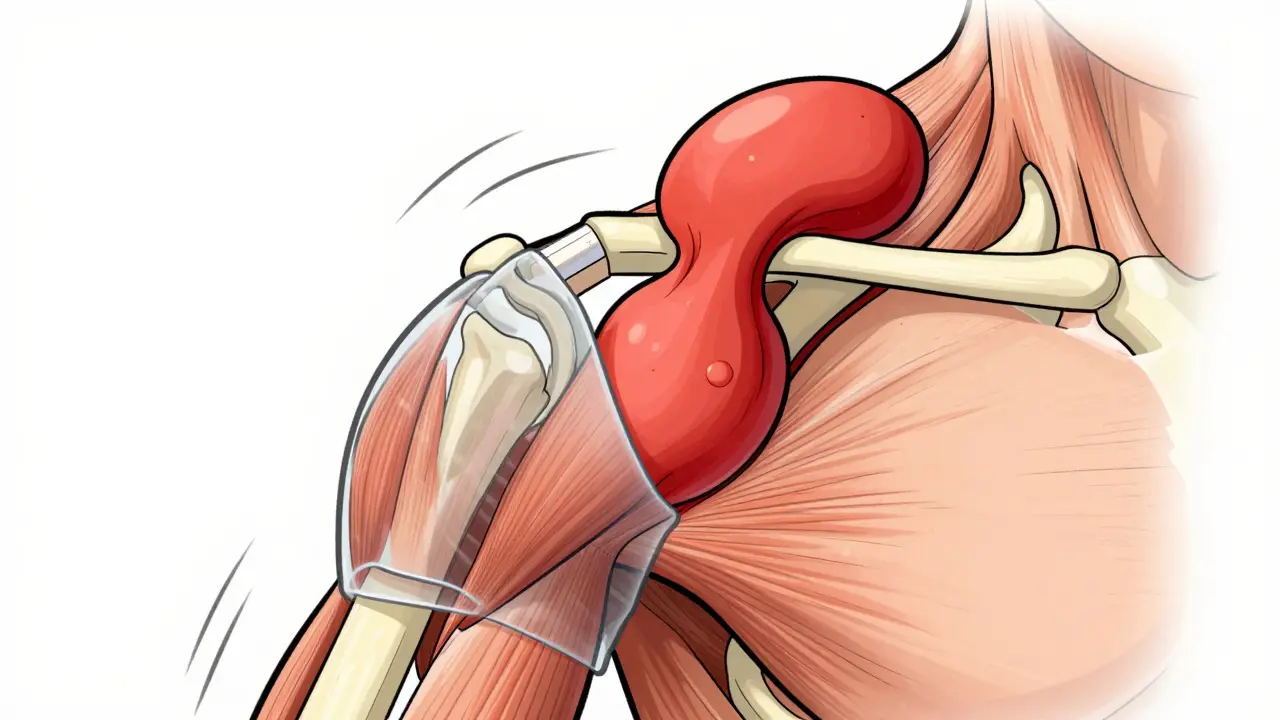
Your shoulder is a ball-and-socket joint, but unlike your hip, it’s not held tightly in place by deep ligaments. Instead, it’s stabilized by four small muscles-the rotator cuff-that wrap around the top of the arm bone like a sleeve. These muscles (supraspinatus, infraspinatus, teres minor, and subscapularis) keep the ball centered when you move your arm. When they get irritated, they swell. That’s rotator cuff tendinitis. It’s not always a tear. In fact, most people with shoulder pain have inflammation, not a full tear. Right above these muscles is a small fluid-filled sac called the subacromial bursa. Think of it like a cushion between the tendons and the bony roof of your shoulder (the acromion). When the tendons are swollen from overuse, they rub against this bursa. The bursa gets inflamed too. That’s bursitis. The two conditions often happen together. You can’t fix one without addressing the other. The classic sign? The painful arc. When you lift your arm out to the side, it hurts between 60° and 120°. That’s when the inflamed tissues get pinched. Pain often gets worse at night, especially if you roll onto that shoulder. Many people wake up because of it.How Common Is This?
About 2 million Americans see a doctor each year for shoulder problems. That number jumps sharply after age 40. By the time you’re 50 to 59, 1 in 5 to 1 in 3 people have some kind of rotator cuff issue. Over 80? That number climbs to more than half. It’s not just aging-repetitive motion matters. Construction workers have a 32% higher risk than the average person. Tennis players, swimmers, painters, and even people who type all day with poor posture are at risk. You don’t need to be an athlete to hurt your shoulder.What Do Doctors Look For?
A good physical exam can tell you a lot. But imaging helps confirm what’s going on. Ultrasound is often the first test. A normal bursa is about 1-2 mm thick. If it’s over 2 mm, that’s a red flag. MRI gives a clearer picture of the tendons themselves-whether they’re frayed, partially torn, or completely gone. But here’s the key point: imaging doesn’t always match symptoms. Some people have big tears on MRI and feel fine. Others have minor changes and are in agony. That’s why treatment focuses on symptoms, not just pictures.First Steps: What You Can Do Right Now
If you’ve just started having shoulder pain, skip the painkillers and the MRI right away. Start here:- Rest-but not too much. Avoid lifting, reaching overhead, or sleeping on the sore side. But don’t stop moving entirely. Keeping the joint moving prevents stiffness.
- Ice it. Apply ice for 15-20 minutes, 3-4 times a day. A bag of frozen peas wrapped in a towel works fine. Ice reduces swelling and numbs the pain.
- Take an NSAID. Ibuprofen (400-600 mg) three times a day for a few days can help. Don’t use it longer than 10 days without talking to your doctor. It’s not a long-term fix.
- Change your habits. If you work at a desk, raise your monitor to eye level. If you carry a bag, switch shoulders. Sleep on your back or the other side. Small changes add up.
When the Pain Won’t Go Away
If you’ve tried the basics for 4-6 weeks and it’s still bothering you, the next step is physical therapy. And yes, it works. Studies show that 80% of people with rotator cuff tendinitis and bursitis improve with rehab alone. No surgery needed. The best rehab programs follow a clear progression:- Start with motion. Pendulum exercises (letting your arm hang and swing gently) begin within days. Do them 3 times a day for 5-10 minutes. This keeps the joint loose without stressing the muscles.
- Move to active motion. After 2-3 weeks, start lifting your arm with help from your other hand or a stick. Don’t force it. Go slow.
- Add resistance. At 4-6 weeks, begin using resistance bands (TheraBand). Focus on external rotation (pulling the band away from your body) and scapular retraction (squeezing your shoulder blades together). Do 3 sets of 15 reps, 5-7 days a week.
- Strengthen, don’t just stretch. Many people focus on stretching, but the real fix is strengthening the muscles that hold the shoulder in place. Weak scapular muscles are a huge contributor to pain.
Corticosteroid Injections: Helpful or Harmful?
If rehab isn’t enough after 6-8 weeks, a corticosteroid injection might be recommended. This is a shot of anti-inflammatory medicine (usually triamcinolone) into the space between the bursa and the bone, guided by ultrasound for accuracy. It works for 65-75% of people, giving relief for 4 to 12 weeks. But here’s the catch: it’s not a cure. It’s a pause button. It gives you a window to do physical therapy without pain. The problem? If you get too many, it can weaken the tendons. Most experts say no more than 2-3 injections per year, with at least 3 months between them. The risk of tendon rupture jumps to 8% with frequent use. And here’s something surprising: a 2022 study in the Journal of Bone and Joint Surgery found that people who got injections and those who only did physical therapy had the same outcomes at 12 months. Surgery didn’t give better results either. So if you’re not improving with rehab, don’t rush to the needle.When Does Surgery Make Sense?
Surgery isn’t the first choice. In fact, it’s the last. Most people never need it. But if you’ve tried 3-6 months of physical therapy, injections, and rest-and you’re still in pain-then arthroscopic subacromial decompression might be considered. This is a minimally invasive procedure where the surgeon removes inflamed tissue (bursectomy) and shaves down part of the acromion bone to create more space. It takes about an hour. Recovery? 4-6 months. Cost? $15,000 to $20,000. But again, studies show that for pure bursitis without a full-thickness tear, surgery offers little advantage over physical therapy. The real surgical candidates are people over 60 with a complete rotator cuff tear. Their healing rate with rehab alone is only 40%. Surgery pushes that to 75%.Real People, Real Results
A 54-year-old carpenter in Sydney stopped working for 3 months because of shoulder pain. He started physical therapy, did his home exercises every day, and returned to full duty after 14 weeks. A 37-year-old tennis player recovered in 10 weeks using a mix of cryotherapy and eccentric strengthening. Both avoided surgery. On the flip side, the biggest reason people end up back in the clinic? The “weekend warrior” effect. They feel better after 6 weeks, go back to lifting weights or playing tennis, and hurt it again. That’s why rehab isn’t just about fixing the shoulder-it’s about changing how you move long-term.What’s New in Treatment?
In 2024, a new ultrasound-guided injection system (AcuNav V) hit the market. It improves accuracy from 72% to 94%, meaning fewer missed shots and less risk of damage. Platelet-rich plasma (PRP) injections are now recommended as a second-line option after steroids fail. A multicenter trial showed PRP worked in 68% of cases, compared to 52% for repeat steroid shots. For older patients, a new technique called blood flow restriction training is showing promise. It uses a cuff to gently restrict blood flow while doing light exercises. It reduces recovery time by 30% for people over 60. And in the next few years, wearable sensors will likely be used to give real-time feedback on exercise form-so you know if you’re doing the move right.What You Can Do Today
If you’re in pain:- Don’t ignore it. The longer you wait, the harder it is to fix.
- Start with rest, ice, and avoiding overhead motion.
- Find a physical therapist who specializes in shoulders. Ask if they use standardized protocols.
- Do your exercises. Every day. Even if it’s just 10 minutes.
- Use a phone app to remind you. One study showed people who used reminders completed 82% of their exercises-compared to 54% without.
- Keep a pain log. Rate your pain on a scale of 0-10. If it goes above 5 during exercise, ease up. Pain is a guide, not a target.
Can shoulder bursitis go away on its own?
Yes, in many cases. Mild bursitis often improves within a few weeks with rest, ice, and avoiding repetitive movements. But if the underlying cause-like poor posture or muscle weakness-isn’t addressed, it usually comes back. That’s why rehab is so important. It’s not just about calming the inflammation; it’s about fixing what caused it.
Is heat or ice better for shoulder pain?
Use ice in the first few days or after activity to reduce swelling. After the acute phase (usually after 3-5 days), heat can help loosen stiff muscles before exercise. But don’t use heat if the area is still swollen or hot to the touch. Heat can make inflammation worse.
How long does shoulder rehab take?
Most people see improvement in 4-6 weeks, but full recovery takes 8-12 weeks. Some cases, especially in older adults or those with chronic issues, can take up to 6 months. The key is consistency. Doing your exercises 5-7 days a week matters more than how long each session lasts.
Should I stop working out if I have shoulder pain?
Not necessarily. Avoid movements that cause pain, especially overhead presses, pull-ups, or heavy lifting. But you can still do lower body workouts, core work, and light cardio. Staying active helps circulation and prevents stiffness. A physical therapist can help you modify your routine so you don’t aggravate the shoulder.
Can poor posture cause shoulder bursitis?
Absolutely. Slouching or having forward shoulders changes the position of the shoulder blade, which reduces the space under the acromion. This makes the rotator cuff and bursa more likely to get pinched. Correcting posture isn’t just about looking better-it’s a core part of treatment.
Are corticosteroid injections dangerous?
When used properly, they’re safe and effective. But repeated injections (more than 2-3 per year) can weaken tendons and increase the risk of rupture. They’re meant to give you a break to do rehab-not to be a permanent solution. Always combine them with physical therapy.
What’s the best sleeping position for shoulder pain?
Sleep on your back with a pillow under the affected arm to keep it slightly elevated. If you must sleep on your side, put a pillow between your arms to keep your shoulder from rolling inward. Avoid sleeping directly on the painful shoulder.
Can I prevent shoulder pain in the future?
Yes. Keep doing the exercises even after you feel better. Strengthen your rotator cuff and scapular muscles 2-3 times a week. Maintain good posture. Avoid sudden increases in overhead activity. And if you’re in a job or sport that stresses the shoulder, take regular breaks and stretch.













Comments (13)